Key Takeaways
- Up to 80% of pink eye cases are viral — antibiotic eye drops don't help these and may delay healing.[4]
- Even bacterial conjunctivitis is self-limited in about 60% of cases without any treatment.[2]
- A Cochrane review of 21 RCTs (8,805 patients) found antibiotics modestly speed bacterial conjunctivitis recovery by 26%.[1]
- Better diagnosis — including telehealth photo assessment — could prevent an estimated 1.1 million inappropriate antibiotic prescriptions per year in the US.[2]
- Watchful waiting with a delayed prescription is a reasonable strategy for typical bacterial pink eye without red flags.[3]
The Pink Eye Antibiotic Reflex
Pink eye is one of the most common reasons adults seek same-day care. A red, irritated eye with discharge sends people to urgent care, primary care, and telehealth visits by the millions every year.
The reflex response in many clinics is simple: write a prescription for antibiotic eye drops and send the patient home. It feels safe, and the patient walks out with a treatment in hand.
But current evidence shows that reflex is usually unnecessary — and sometimes counterproductive. Most pink eye in adults is viral, and antibiotics do not work on viruses. Prescribing them anyway exposes you to side effects without benefit and can mask the actual diagnosis.
The diagnostic step that separates "needs antibiotics" from "needs supportive care" is mostly a matter of history and a clear look at the eye. Telehealth has made that easier with photo-based assessment.
The Big Picture: What Causes Pink Eye in Adults
Conjunctivitis falls into a handful of categories, and each one calls for a different approach. Sorting them apart is where most of the work happens.
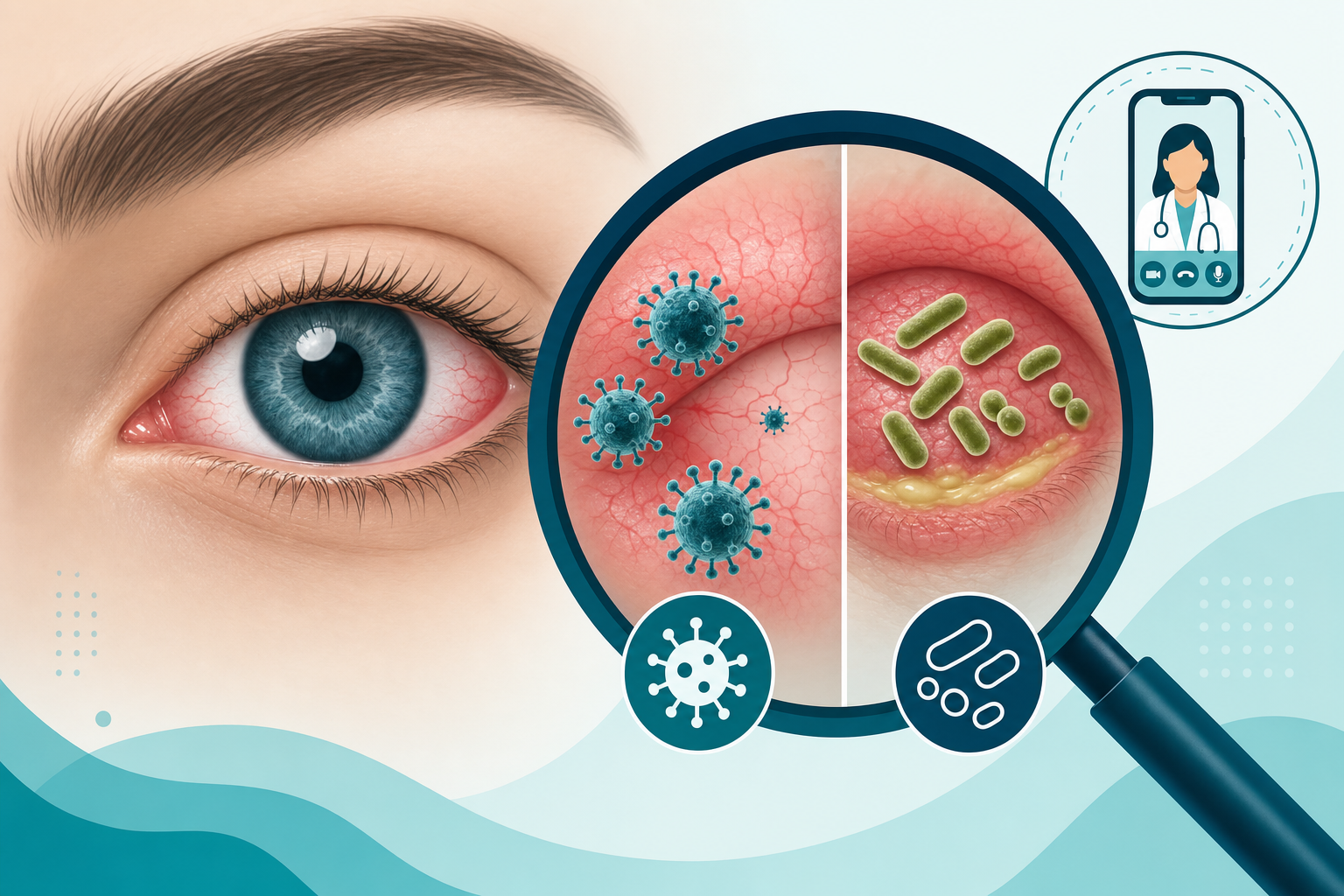
Viral conjunctivitis (up to 80% of infectious cases)
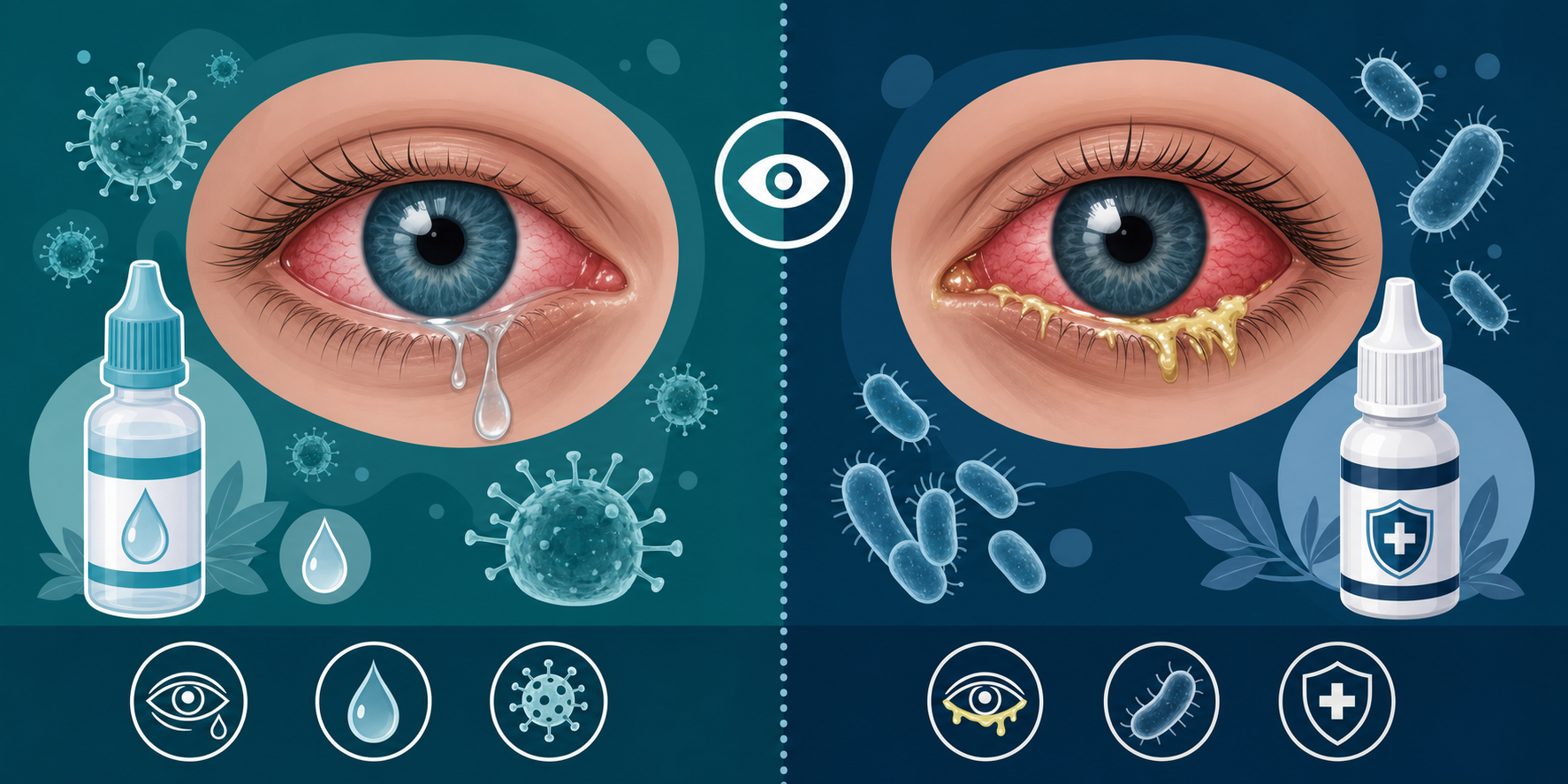
Viral pink eye is the most common form by a wide margin. Adenoviruses are responsible for 65–90% of viral cases in adults.[4] It often shows up alongside a head cold, sore throat, or known sick contacts. The discharge is typically watery and clear, and the redness may start in one eye and spread to the other within a few days. Symptoms run their course in one to two weeks without treatment.[7]
Bacterial conjunctivitis (~20% of infectious cases)
Common pathogens include Staphylococcus, Streptococcus, and Haemophilus influenzae. The hallmark is mucopurulent discharge — thick, sticky, often yellow or green — that may glue the eyelids shut overnight. About 60% of uncomplicated bacterial cases clear on their own within 5–7 days.[2]
Allergic conjunctivitis
No infection involved. Itchy, watery, bilateral eyes that often arrive with sneezing, nasal congestion, or other allergy symptoms. Antihistamine drops handle most cases.
Hyperacute bacterial conjunctivitis (rare but urgent)
Caused by Neisseria gonorrhoeae. It produces copious purulent discharge within 24 hours of onset and can threaten the cornea. This presentation needs IM ceftriaxone and urgent in-person evaluation.[3]
What the Evidence Says About Antibiotics
The strongest data on antibiotic eye drops comes from a 2024 Cochrane review. It pooled 21 randomized controlled trials with 8,805 participants who had acute bacterial conjunctivitis.[1]
In the intention-to-treat analysis, antibiotics increased clinical recovery by 26% at end of therapy (RR 1.26; 95% CI 1.09–1.46) — a moderate-certainty finding. In lab-confirmed bacterial cases, the likelihood of microbiological cure was 53% higher with antibiotics.[1]
That sounds like a clear win — but the catch is the diagnosis itself. Bacterial pathogens are isolated in only about 50% of cases that clinicians suspect are bacterial.[2] The other half is usually viral. So when a clinic prescribes drops for every "pink eye," roughly half of those prescriptions are aimed at a target that isn't there.
Antibiotic drops also carry small but real risks: ocular irritation, allergic reactions, and the potential to delay recognition of a different diagnosis. The better strategy is the one the data supports: differentiate viral from bacterial first, then decide.
Watchful Waiting: A Reasonable Approach
For typical bacterial pink eye without red flags, current evidence supports a delayed-prescription strategy. The setup is straightforward: the patient receives a prescription but is asked to wait roughly 3 days before filling it.
If symptoms improve on their own — about a 60% chance — they avoid antibiotics entirely.[2] If symptoms worsen or stall, they fill the prescription. The safety net stays in place, and unnecessary drops get avoided in cases that would have resolved anyway.
The 2024 American Academy of Ophthalmology Preferred Practice Pattern reflects this. Antibiotics are a discretionary recommendation in routine bacterial conjunctivitis: the benefit is real, but the trade-offs are close enough that watchful waiting is a defensible choice in many cases.[3]
| Pink Eye Type | Cause | Typical Discharge | First-Line Approach | When to Escalate |
|---|---|---|---|---|
| Viral | Adenoviruses (65–90%) | Watery, clear | Supportive care: cold compresses, artificial tears, hygiene | Severe symptoms, prolonged course, photophobia |
| Mild bacterial | Staph, Strep, H. influenzae | Mucopurulent, sticky | Watchful waiting or delayed prescription | No improvement at 3–5 days |
| Moderate bacterial | Same | Heavier purulent | Topical antibiotic (e.g., erythromycin, polymyxin-trimethoprim) | No improvement at 48–72 hours |
| Hyperacute | Neisseria gonorrhoeae | Copious, rapid onset | URGENT in-person care | Immediate (vision-threatening) |
| Allergic | Histamine release | Watery, itchy | Antihistamine drops (olopatadine) | Severe vision change or pain |
Where Telehealth Fits
Pink eye is well-suited to photo-based or video-based assessment. The most important diagnostic information — discharge type, redness pattern, eyelid involvement, symptom timeline — can be conveyed without a slit lamp.
A 2024 study showed that smartphone photographs reliably support clinical assessment of acute bacterial conjunctivitis.[5] A 2023 telemedicine eye health screening study reported 72.2% sensitivity for infective conjunctivitis through remote eye examination.[6]
In a virtual visit, the physician can:
- Compare discharge type (watery vs. purulent) on a high-quality photo
- Assess redness pattern and unilateral vs. bilateral involvement
- Take a structured history of onset, contact lens use, sick contacts, and allergies
- Screen for red flags requiring in-person referral
- Issue a delayed prescription or a supportive care plan
For most adults with uncomplicated pink eye, this is faster than an in-person appointment — and particularly useful for confirming that the diagnosis is not urgent.
What This Means for You
If your symptoms are mild and your discharge is watery, your pink eye is most likely viral. Cold compresses, artificial tears, and good hand hygiene are the treatment. Antibiotic drops will not speed it up.
If your discharge is thick and yellow or green, it may be bacterial — but most cases still resolve on their own within a week. A clinician can talk you through watchful waiting before defaulting to antibiotic drops.
If you wear contact lenses, this is a different conversation. Stop wearing them and get evaluated — bacterial keratitis from Pseudomonas is a serious concern in lens wearers and can threaten vision.
A telehealth visit can usually sort which category you're in within a few minutes, and you'll walk away with a clear plan instead of an automatic prescription.
Red Flags: Always See a Doctor in Person
Some symptoms move pink eye out of the routine category and into something that needs hands-on examination. Get in-person care for any of these:
- Severe eye pain (not just irritation or grittiness)
- Vision changes or blurry vision that doesn't clear with blinking
- Sensitivity to light beyond mild discomfort
- Contact lens wearer with a red eye
- Recent eye surgery or eye trauma
- Copious purulent discharge developing within 24 hours (concern for gonococcal infection)
- Symptoms not improving after 5–7 days
- Immunocompromised patient with a red eye
References
- Honkila M, Koskela U, Kontiokari T, et al. "Effect of Topical Antibiotics on Acute Bacterial Conjunctivitis: A Systematic Review and Meta-analysis." Ophthalmology (Cochrane update). 2024. pubmed.ncbi.nlm.nih.gov
- Azari AA, Barney NP. "Conjunctivitis: A Systematic Review of Diagnosis and Treatment." JAMA. 2013;310(16):1721-1729. pmc.ncbi.nlm.nih.gov
- American Academy of Ophthalmology. "Conjunctivitis Preferred Practice Pattern." 2024. guidelinecentral.com
- "Viral Conjunctivitis: Update on Diagnosis and Management." Microorganisms. 2025. pmc.ncbi.nlm.nih.gov
- "Smartphone Photograph-Based Assessment of Acute Bacterial Conjunctivitis." 2024. pubmed.ncbi.nlm.nih.gov
- "Telemedicine-Enabled Eye Health Screening: Diagnostic Accuracy Study." Eye. 2023. pmc.ncbi.nlm.nih.gov
- Cronau H, Kankanala RR, Mauger T. "Diagnosis and Management of Red Eye in Primary Care." American Family Physician. 2010;81(2):137-144. aafp.org